
Every year, around this time, benchmark reports from MGMA, Doximity, Medscape, and others provide a snapshot of physician compensation. They’re all helpful reference points, giving you a general sense of how physician pay is changing on an average each year. But while these numbers update once a year, physician compensation is a lot more dynamic, influenced by local market conditions, and is different for each individual. Relying on just static averages can quickly fall out of step with reality.
This is why we started the anonymous salary-sharing project on Marit. It’s clinician-powered, by and for clinicians. Marit shows real, anonymized, verified, individual-level data; and not just the averages, but with all the details that matter: bonuses, comp models, benefits, shifts, wRVU thresholds, and more.
The Problem with Averages
The issue with all these medians and averages is that they don’t apply to anyone individually. Each of us has a unique practice structure, work structure and preferences – and our salaries reflect the combination of all those factors. The details behind each individual salary matters. And if everyone was paid at the median, today’s median will become tomorrow’s 90th percentile.
Indeed, based on the physician salary data on Marit – salary differences within a specialty can be as pronounced as those across different specialties. Physicians in the top 10% often earn 1.5 – 3.5 times more than those in the bottom 10%.
We first heard about this idea of intraspecialty variance from Dr. Jim Dahle’s post at the White Coat Investor. Let’s dig into this.
Yes, there is wide variation across specialties – you can see that in the spread of the larger green dots, which show median salaries by specialty. But what’s even more striking is the variation within each specialty. The smaller dots show the 10th and 90th percentiles; and in many cases, they’re very far apart.
Yes, on average, Family Medicine salaries are lower than those of their peers in procedural fields like Orthopedic Surgeons, but there are many Family medicine salaries that are higher than Orthopedic Surgeon salaries on Marit.
Similarly, there are Emergency Medicine physician salaries that exceed Oncologist salaries, especially in independent or high-volume groups. And Hospitalist salaries, especially with night or ICU coverage, outpace Plastic Surgeon salaries working in academic or low-volume settings. The comparisons can go on.
Specialties With the Most Variability
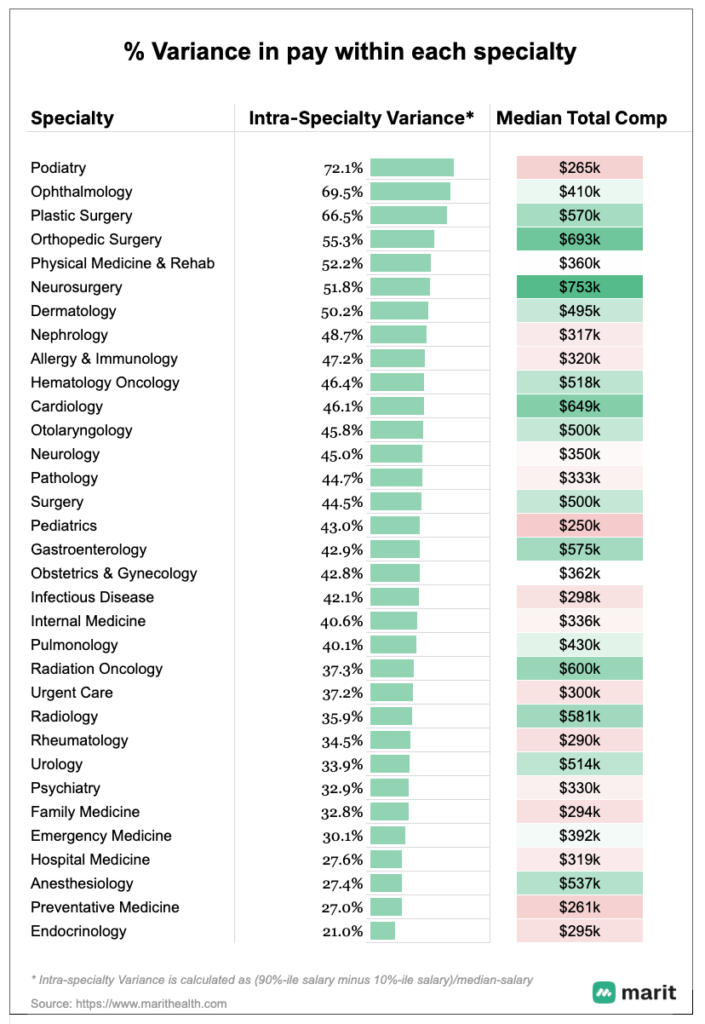
So, which specialties have the highest variance in pay? It turns out, there is little to no correlation between a specialty’s median salary and how widely incomes can vary within it.
Take Podiatry salaries, for example. The median is relatively low at $265k, but it ranks highest in terms of intra-specialty variance. That’s because some self-employed podiatrists earn well into the seven figures. As this respondent reported – “Self-employed. Solo practice. I know I’m an outlier, and I do a lot of non-mainstream podiatry things, but it’s worked out well. Best year was $2M.”
It’s a powerful reminder that individual choices can dramatically shape outcomes. Knowing how others have structured their careers can help know what’s possible.
Other specialties with high variance include:
- Ophthalmologist salaries have a 70% spread between the 10th and 90th percentile, as there is a significant difference between the earning potential of self-employed and private medical group ophthalmologists, especially when they perform high-volume procedures or have equity in their practices, relative to their hospital-based counterparts.
- Orthopedic Surgery salaries, where compensation often depends on the ownership structure. Surgeons who are partners in an ASC (ambulatory surgery center) or generate high wRVUs can earn significantly more than employed surgeons on a base-plus-bonus model.
- Neurologist salaries, where the variance reflects a mix of general outpatient practice, subspecialty expertise (like epilepsy or stroke), and procedure-based work (e.g., EMG, Botox, intraoperative monitoring). Academic neurologists tend to earn less, while those in private or hybrid models with high patient volumes can earn much more.
- Allergist salaries vary significantly by setting. Physicians in academic roles typically earn far less than those in private practice, where procedure volume can be quite high.
On the other end of the spectrum, the specialties with the least variance tend to fall into two categories: hospital-based roles and preventive-care specialties.
Hospital-based fields like Anesthesiology, Hospital Medicine, Emergency Medicine, and even Radiology often have standardized compensation structures, especially in large health systems. These roles are frequently salaried, with limited variability in ownership, bonus upside, or procedure-based pay. See our post on compensation models here for more details.
Preventive and lower-acuity fields, such as Preventative Medicine salaries, Endocrinologist salaries, Psychiatrist salaries, etc., also show lower variance, often due to employed positions with consistent workloads and fewer opportunities for high-volume procedural income. Compensation tends to be more predictable and stable.
Intra-specialty variance is calculated as (90th percentile salary – 10th percentile salary) ÷ median salary.
Why This Matters
This matters for two reasons –
We can review where we fall within the salary spectrum of our specialty, ensure fair compensation and identify potential areas for change.
But more importantly, we can all learn from each other on what’s possible. Recognize what’s achievable financially and professionally, so we can make more empowered career decisions. There are hundreds of choices we will make throughout our career – where to work, how much to work, what kind of practice to join; and each of those will shape our income, personal life, and career satisfaction in different ways.
The detailed, anonymized, salaries contributed by the community on Marit reflects the diverse choices others have made. And it helps us all learn what’s possible. So we can our individual careers with clarity.
If you’d like to support the Pay Transparency project for medicine, please add your anonymous salary on Marit here.
About the Data & Methodology
Marit’s Data is different. It is –
Unique – since it captures the compensation data along with all the details that matter – bonuses, shifts, schedules, benefits, and more
Comprehensive – Across all specialties and Professions (Physicians & APPs), Employer Types (large and small, including Self-employed, Academic & Non Academic), Job Types (Full Time, Part Time, PRNs and Locums) and Employment Types (W-2, 1099, K-1)
Current – Unlike other benchmarks that only update their data once a year, all salaries reflect the clinician’s current compensation, and all averages are updated in real-time as new salaries are added
All data in this report comes from anonymized salary contributions on Marit, as of May, 2025. Only verified salary reports approved by our moderation team are included.

